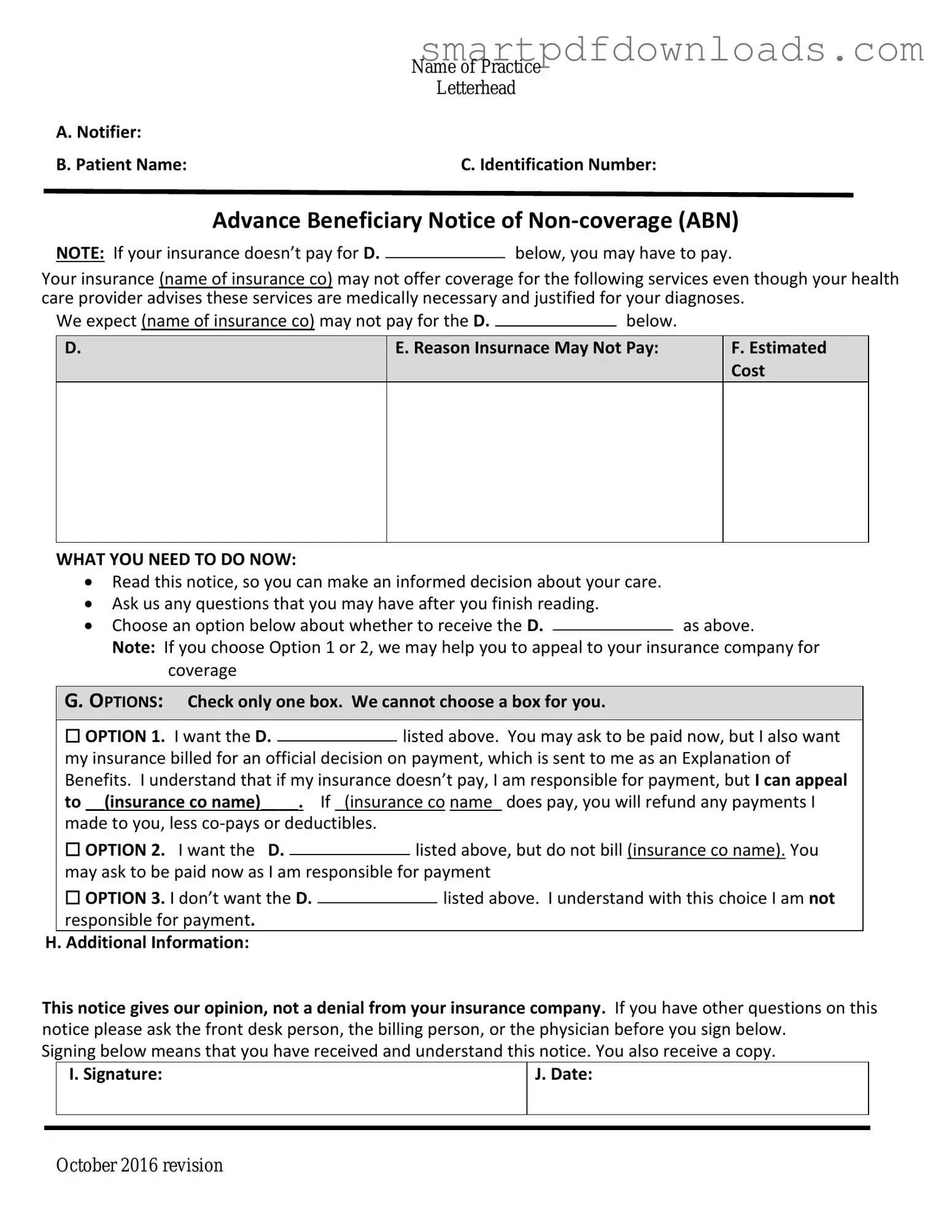
Advance Beneficiary Notice of Non-coverage Form
Advance Beneficiary Notice of Non-coverage Form
Florida Realtor Lease Agreement - Transparency in payment responsibilities ensures that tenants are aware of their financial obligations under the lease.
A New York Non-disclosure Agreement (NDA) is a legal document that establishes a confidential relationship between parties, ensuring that sensitive information remains protected. This form is crucial for businesses and individuals who wish to share proprietary information without the risk of it being disclosed to unauthorized third parties. For more details on how to create this important document, you can visit nypdfforms.com/non-disclosure-agreement-form/. Understanding the key components of an NDA can help safeguard valuable ideas and trade secrets.
Fedex Informed Delivery - Each package requires a separate Release Authorization form.
|
Name of Practice |
|
Letterhead |
A. Notifier: |
|
B. Patient Name: |
C. Identification Number: |
Advance Beneficiary Notice of
NOTE: If your insurance doesn’t pay for D.below, you may have to pay.
Your insurance (name of insurance co) may not offer coverage for the following services even though your health care provider advises these services are medically necessary and justified for your diagnoses.
We expect (name of insurance co) may not pay for the D. |
|
below. |
|
D.
E. Reason Insurnace May Not Pay:
F.Estimated Cost
WHAT YOU NEED TO DO NOW:
Read this notice, so you can make an informed decision about your care.
Ask us any questions that you may have after you finish reading.
Choose an option below about whether to receive the D.as above.
Note: If you choose Option 1 or 2, we may help you to appeal to your insurance company for coverage
G. OPTIONS: Check only one box. We cannot choose a box for you.
|
☐ OPTION 1. I want the D. |
|
listed above. You may ask to be paid now, but I also want |
||||
|
|
||||||
|
my insurance billed for an official decision on payment, which is sent to me as an Explanation of |
||||||
|
Benefits. I understand that if my insurance doesn’t pay, I am responsible for payment, but I can appeal |
||||||
|
to __(insurance co name)____. If _(insurance co name_ does pay, you will refund any payments I |
||||||
|
made to you, less |
|
|
|
|||
|
☐ OPTION 2. I want the D. |
|
|
listed above, but do not bill (insurance co name). You |
|||
|
|
|
|||||
|
may ask to be paid now as I am responsible for payment |
||||||
|
☐ OPTION 3. I don’t want the D. |
|
|
|
listed above. I understand with this choice I am not |
||
|
|
|
|
||||
|
responsible for payment. |
|
|
|
|||
H. Additional Information: |
|
|
|
||||
This notice gives our opinion, not a denial from your insurance company. If you have other questions on this notice please ask the front desk person, the billing person, or the physician before you sign below.
Signing below means that you have received and understand this notice. You also receive a copy.
|
I. Signature: |
J. Date: |
|
|
|
|
|
|
October 2016 revision
Once you have the Advance Beneficiary Notice of Non-coverage form in hand, it is essential to fill it out accurately. This form is crucial for understanding your financial responsibilities regarding healthcare services. Follow these steps to ensure that you complete the form correctly.
After completing the form, ensure that the patient receives a copy for their records. This step is vital in maintaining transparency and clarity regarding healthcare services and potential costs.
The Advance Beneficiary Notice of Non-coverage (ABN) form is often misunderstood. Here are four common misconceptions:
This is not necessarily true. The ABN is a notification that Medicare may not cover a specific service, but it does not guarantee non-coverage. It simply informs beneficiaries that they may be responsible for payment if Medicare denies the claim.
Signing the ABN does not automatically mean you agree to pay for the service. It indicates that you understand the potential for non-coverage, but you still have the right to appeal any denial of payment.
ABNs can be issued for any service that may not be covered, even if it is commonly covered. Providers issue them when they believe that a service may not meet Medicare's coverage criteria.
This is incorrect. Beneficiaries in Medicare Advantage Plans can also receive ABNs. The form serves the same purpose regardless of whether you are in Original Medicare or a Medicare Advantage Plan.
The Advance Beneficiary Notice of Non-coverage (ABN) form is an important document used in healthcare settings. It informs patients when a service or item may not be covered by Medicare. Along with the ABN, there are several other forms and documents that may be utilized to ensure clarity and compliance in the healthcare process. Below is a list of these documents, each serving a specific purpose.
Understanding these documents can help patients navigate their healthcare options and responsibilities more effectively. Each form plays a critical role in ensuring transparency and communication between healthcare providers and patients.