Cna Shower Sheets Form
Cna Shower Sheets Form
Fedex Informed Delivery - Delivery will be attempted only with the Release Authorization in place.
When navigating the paperwork involved in motorcycle ownership, understanding the essential aspects of a Motorcycle Bill of Sale is crucial. This specific form acts as an essential tool for documenting the transaction, ensuring both parties agree on the details of the sale. For further insights, consider reviewing our comprehensive guide on the Motorcycle Bill of Sale.
How to Set Up March Madness Bracket - Challenge yourself to predict the unexpected twists in the tournament.
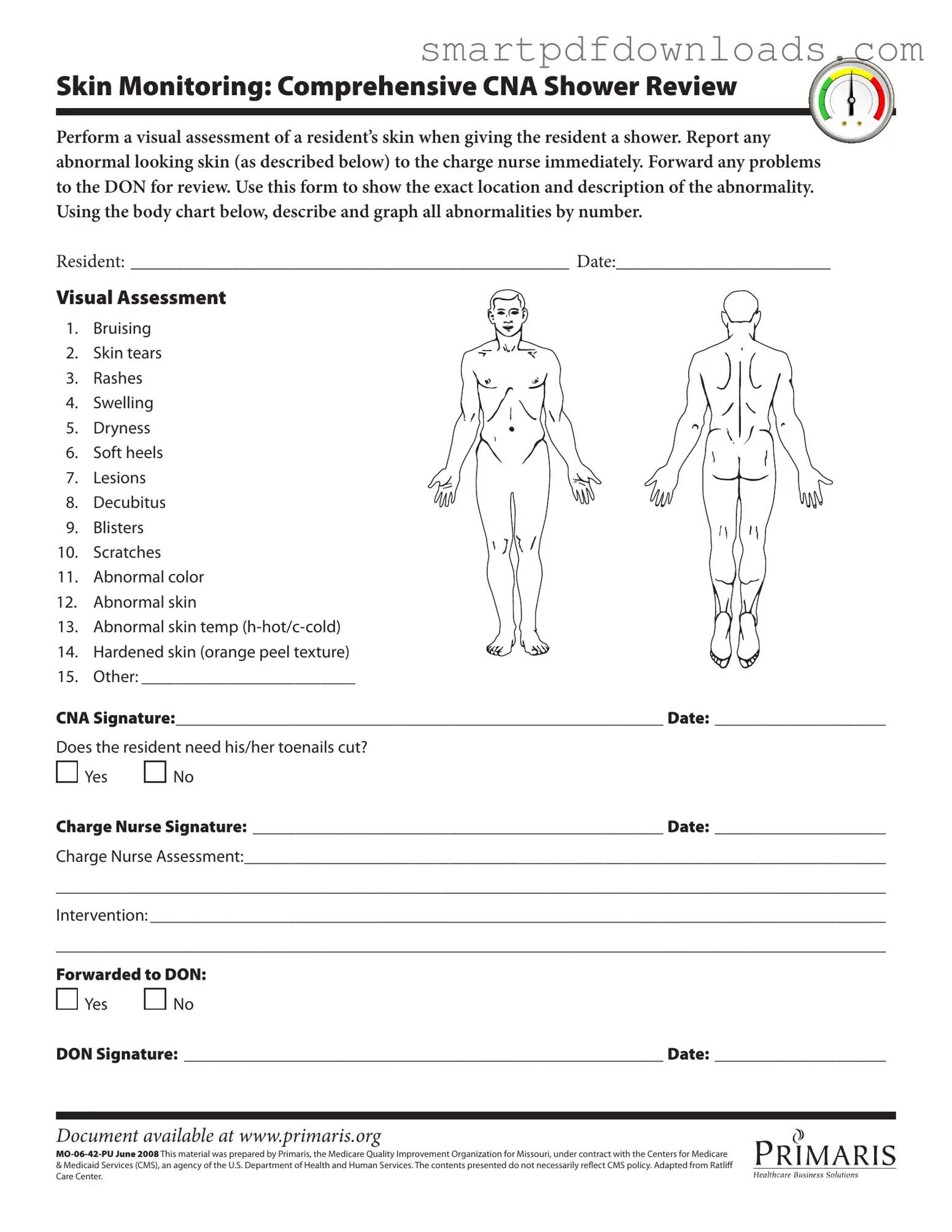
Skin Monitoring: Comprehensive CNA Shower Review
Perform a visual assessment of a resident’s skin when giving the resident a shower. Report any abnormal looking skin (as described below) to the charge nurse immediately. Forward any problems to the DON for review. Use this form to show the exact location and description of the abnormality. Using the body chart below, describe and graph all abnormalities by number.
RESIDENT: _______________________________________________ DATE:_______________________
Visual Assessment
1. Bruising
2. Skin tears
3. Rashes
4. Swelling
5. Dryness
6. Soft heels
7. Lesions
8. Decubitus
9. Blisters
10. Scratches
11. Abnormal color
12. Abnormal skin
13. Abnormal skin temp
14. Hardened skin (orange peel texture)
15. Other: _________________________
CNA Signature:_________________________________________________________ Date: ____________________
Does the resident need his/her toenails cut?

 Yes
Yes 
 No
No
Charge Nurse Signature: ________________________________________________ Date: ____________________
Charge Nurse Assessment:___________________________________________________________________________
_________________________________________________________________________________________________
Intervention: ______________________________________________________________________________________
_________________________________________________________________________________________________
Forwarded to DON:

 Yes
Yes 
 No
No
DON Signature: ________________________________________________________ Date: ____________________
Document available at www.primaris.org
&Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily relect CMS policy. Adapted from Ratlif Care Center.
Completing the CNA Shower Sheets form is essential for documenting the skin assessment of a resident during a shower. This process ensures that any abnormalities are reported and addressed appropriately. Follow the steps below to accurately fill out the form.
This form is designed to document all types of skin conditions, not just severe ones. It includes various categories like bruising, dryness, and rashes, which are important for overall skin health.
While the charge nurse plays a crucial role, the information is also forwarded to the Director of Nursing (DON) for further review. This ensures a comprehensive approach to skin monitoring.
The CNA's role is to observe and report. Treatment decisions and interventions are made by the charge nurse or DON based on the documented observations.
The body chart is a vital part of the form. It allows for precise documentation of the location and nature of skin abnormalities, which is essential for effective monitoring.
All residents should be assessed during showers, regardless of their previous skin conditions. Early detection of any changes can prevent more serious problems.
While it may seem like an extra step, completing the form is a quick process that enhances the quality of care. It ensures that important information is communicated effectively.
Although the form is used during showers, the information gathered can inform care outside of showering times. It contributes to a resident’s overall care plan.
In a healthcare setting, particularly in facilities where residents receive assistance with daily activities, several forms and documents accompany the CNA Shower Sheets. Each of these documents serves a specific purpose in ensuring the health and safety of residents while maintaining comprehensive records of their care. Below is a list of commonly used forms that complement the CNA Shower Sheets.
These documents, when used alongside the CNA Shower Sheets, create a comprehensive picture of each resident's care. They help to ensure that all aspects of a resident's health and well-being are monitored and addressed, promoting a safe and supportive environment in healthcare facilities.