Free Living Will Form
Free Living Will Form
Letter of Intent to Sue Example - This document should be kept for records in case of future disputes or negotiations.
By utilizing the Durable Power of Attorney, you can ensure that your designated agent is empowered to handle your affairs in accordance with your wishes, thereby providing peace of mind and clarity during uncertain times.
Temporary Guardianship Form California Pdf - The Temporary Custody form helps establish trust among families during critical times.
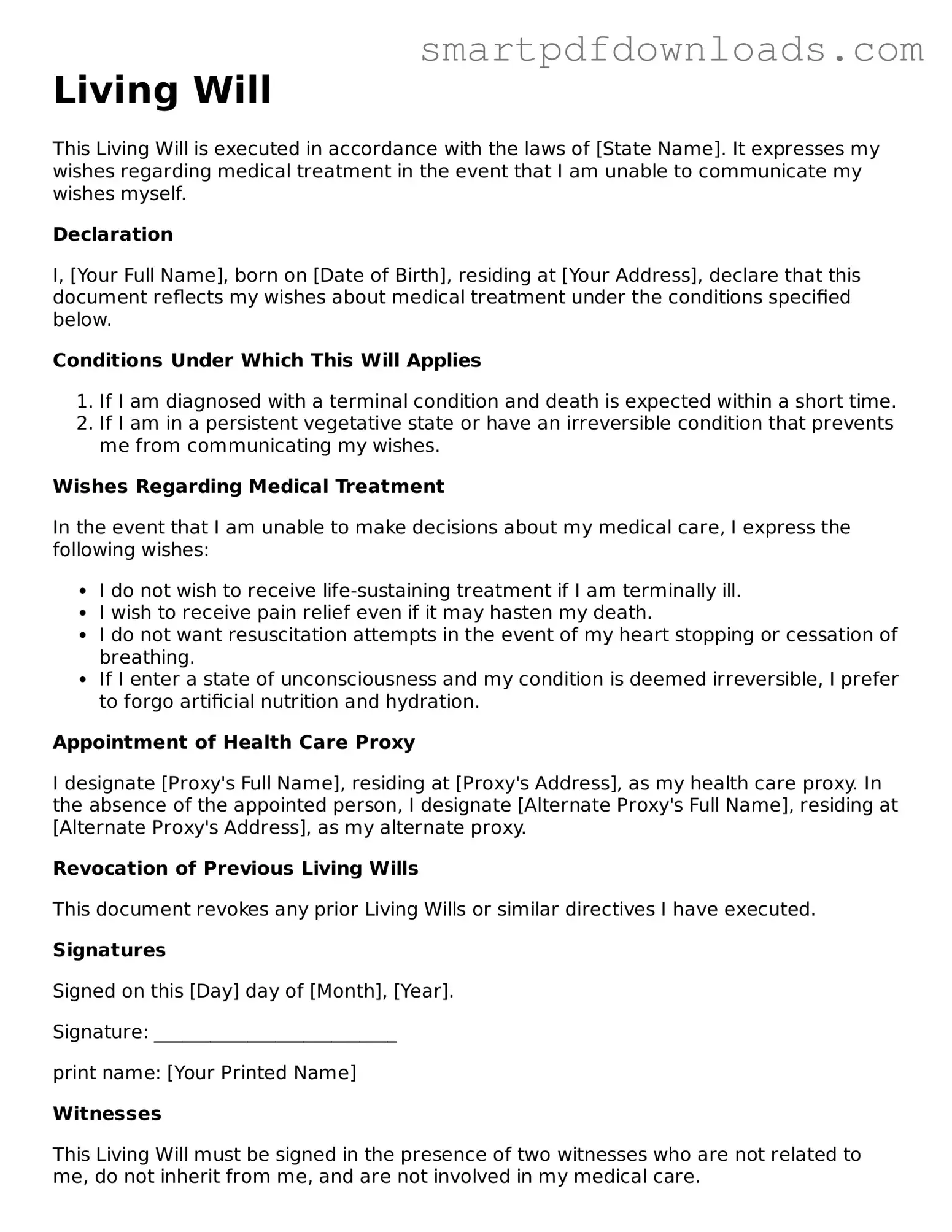
Living Will
This Living Will is executed in accordance with the laws of [State Name]. It expresses my wishes regarding medical treatment in the event that I am unable to communicate my wishes myself.
Declaration
I, [Your Full Name], born on [Date of Birth], residing at [Your Address], declare that this document reflects my wishes about medical treatment under the conditions specified below.
Conditions Under Which This Will Applies
Wishes Regarding Medical Treatment
In the event that I am unable to make decisions about my medical care, I express the following wishes:
Appointment of Health Care Proxy
I designate [Proxy's Full Name], residing at [Proxy's Address], as my health care proxy. In the absence of the appointed person, I designate [Alternate Proxy's Full Name], residing at [Alternate Proxy's Address], as my alternate proxy.
Revocation of Previous Living Wills
This document revokes any prior Living Wills or similar directives I have executed.
Signatures
Signed on this [Day] day of [Month], [Year].
Signature: __________________________
print name: [Your Printed Name]
Witnesses
This Living Will must be signed in the presence of two witnesses who are not related to me, do not inherit from me, and are not involved in my medical care.
Filling out a Living Will form is an important step in expressing your healthcare preferences. This document will guide your loved ones and healthcare providers in making decisions about your medical care if you become unable to communicate your wishes.
Many people have misconceptions about Living Wills that can lead to confusion and misinformation. Here are seven common myths along with clarifications.
A Living Will is an essential document that outlines your preferences regarding medical treatment in the event you become unable to communicate your wishes. However, it is often accompanied by several other important forms and documents that work together to ensure your healthcare decisions are honored. Below is a list of related documents that you may want to consider when preparing your Living Will.
Incorporating these documents alongside your Living Will can create a comprehensive plan for your healthcare and end-of-life wishes. Taking the time to prepare these forms not only provides clarity for your loved ones but also ensures that your preferences are respected when it matters most.