Legal Power of Attorney for a Child Form for the State of New York
Legal Power of Attorney for a Child Form for the State of New York
Temporary Medical Power of Attorney for a Minor - Parents might need this form when they have to leave their child with someone outside the immediate family.
To ensure a smooth transaction when buying or selling a trailer in New York, it's essential to utilize the New York Trailer Bill of Sale form. This document not only verifies the sale but also includes important details that protect both parties involved. As you prepare to complete this form, click here to download the template and facilitate a hassle-free process.
Florida Minor Power of Attorney - This arrangement can provide reassurance for extended family members stepping in.
Do You Need a Lawyer for Power of Attorney - A document that can aid in school enrollment processes for children.
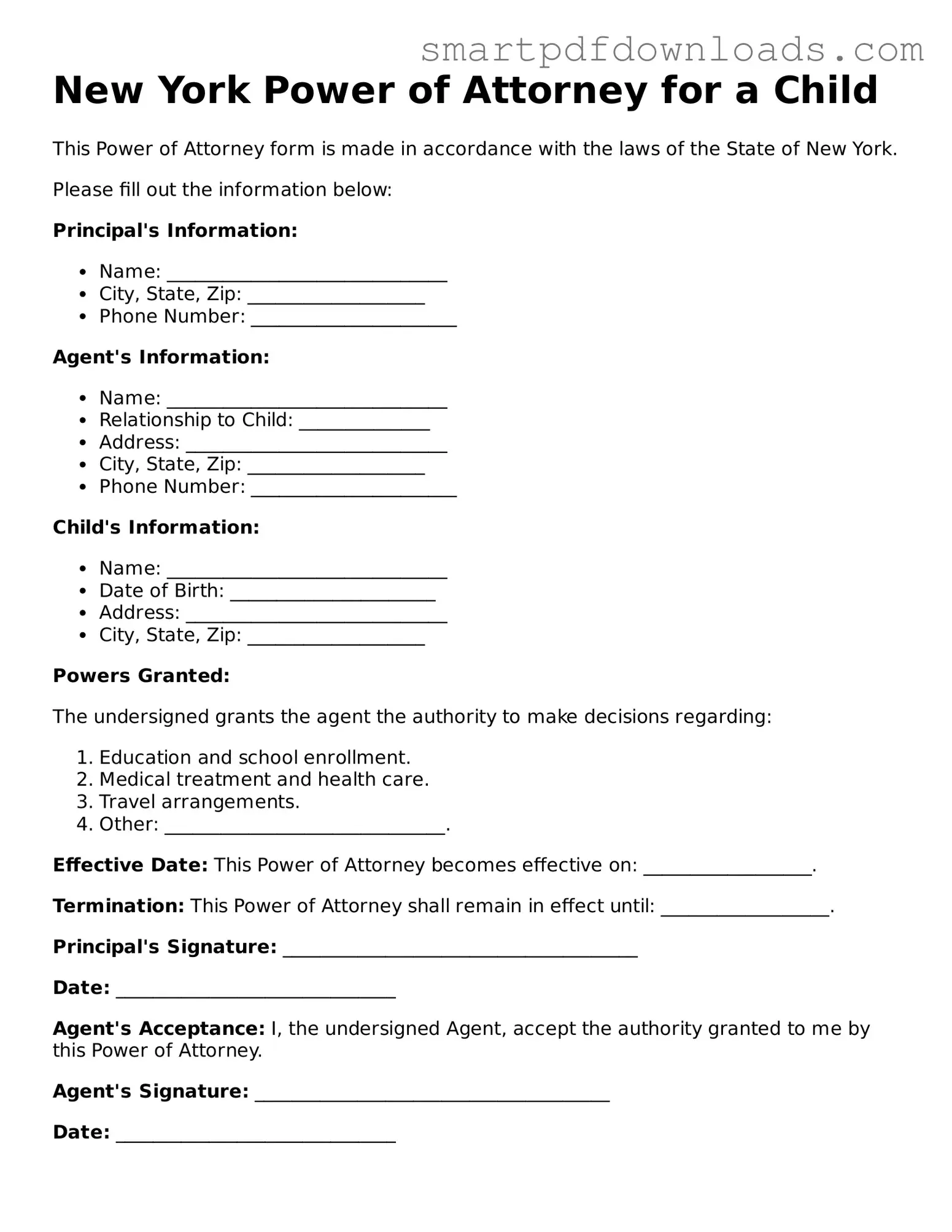
New York Power of Attorney for a Child
This Power of Attorney form is made in accordance with the laws of the State of New York.
Please fill out the information below:
Principal's Information:
Agent's Information:
Child's Information:
Powers Granted:
The undersigned grants the agent the authority to make decisions regarding:
Effective Date: This Power of Attorney becomes effective on: __________________.
Termination: This Power of Attorney shall remain in effect until: __________________.
Principal's Signature: ______________________________________
Date: ______________________________
Agent's Acceptance: I, the undersigned Agent, accept the authority granted to me by this Power of Attorney.
Agent's Signature: ______________________________________
Date: ______________________________
Filling out the New York Power of Attorney for a Child form is an important step for parents or guardians who wish to designate someone else to make decisions on behalf of their child. This process ensures that the designated individual has the authority to act in the best interest of the child when needed. Below are the steps to complete the form accurately.
Once the form is completed and signed, it is advisable to inform the designated person of their responsibilities and ensure they understand the powers granted. This clarity will help in managing the child's needs effectively.
Understanding the New York Power of Attorney for a Child form is essential for parents and guardians. However, several misconceptions can lead to confusion. Here are eight common misconceptions, along with clarifications to help you navigate this important legal document.
By addressing these misconceptions, you can better understand the New York Power of Attorney for a Child form and its implications for your family. It is always wise to consult with a legal professional if you have questions or concerns.
When preparing a Power of Attorney for a Child in New York, several other forms and documents may be beneficial to ensure comprehensive care and legal authority. Each of these documents serves a specific purpose and can help clarify responsibilities and rights. Here’s a list of commonly used forms that complement the Power of Attorney for a Child.
Having these documents prepared alongside the Power of Attorney for a Child can help ensure that the designated agent has the necessary authority and information to act in the child's best interest. It promotes clarity and peace of mind for everyone involved.